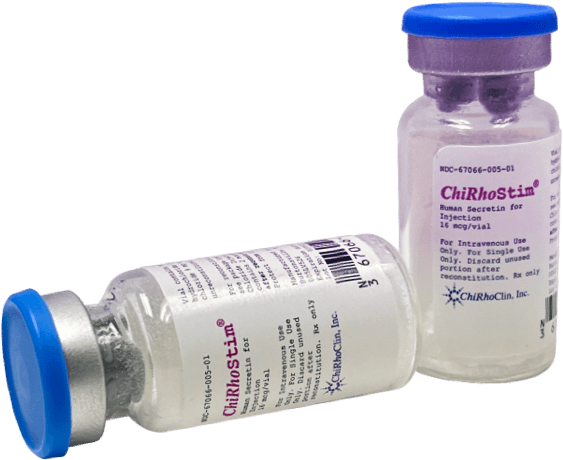
Human Secretin for Injection
Secretin is a naturally occurring 27-amino acid peptide released by ductal mucosa in response to acid in the lumen; It works by stimulating the pancreas to secrete fluid within one minute of injection, mimicking the natural secretin stimulation in response to the emptying of the stomach.
The FDA approved indications for Human Secretin:
- Exocrine Pancreas Function Test;
- Zollinger-Ellison Syndrome Test, and
- Stimulation of pancreatic secretions to facilitate the identification of the ampulla of Vater and accessory papilla during endoscopic retrograde cholangio-pancreatography (ERCP).

The ChiRhoStim® Advantage
- ChiRhoStim® is reimbursable with J-Code 2850.
- ChiRhoStim® is fast acting and easy to use.
- ChiRhoStim® has flexible storage ranges:
5 years at freezer (-20°C)
2 years at refrigerated (5 ° C)
2 years at room temperature (25 ° C) conditions - ChiRhoStim® is Pyxis MedStation compatible.

How does it work?
Secretin is a naturally occurring 27-amino acid peptide released by ductal mucosa in response to acid in the lumen; It works by stimulating the pancreas to secrete fluid within one minute of injection, mimicking the natural secretin stimulation in response to the emptying of the stomach.
Highly purified synthetic peptide, ChiRhoStim® Human Secretin for Injection is the most sensitive and accurate for testing because it increases bicarbonate and pancreatic fluid secretion by the exocrine cells, it also relaxes the sphincter of Oddi and opens pancreatic duct orifices.
Injected intravenously at the time of imaging (MRCP), images are then taken every 30 seconds for 10 minutes. Maximum output of pancreatic fluid is optimal between 6 to 8 minutes. A dynamic image and video is created from a 3-D rendering by the radiologist. This image sequence examines the pancreas response to stimulation. The excess pancreatic fluid/bicarbonate will resonate a sharper image of the pancreas. You are turning static MRCP’s into dynamic images with pancreatic stimulation.
Applications
ChiRhoStim® (Human Secretin for Injection) is approved for the diagnostic indications of exocrine pancreas function test, facilitated cannulation during ERCP procedures, and Zollinger-Ellison Syndrome test.
EPFT
Direct pancreatic function testing is considered the “surrogate” gold standard because obtaining pancreatic tissue from biopsy specimens carries a significant risk of complications. Because subtle functional changes occur at an early stage of fibrosis, direct PFTs may be the most sensitive diagnostic tests for early CP. PFTs are usually unnecessary for the diagnosis of advanced CP, because imaging tests often reveal typical structural changes. However, the diagnosis of early CP can be challenging, as these features may not always be apparent. The ePFT compares well with the traditional PFT.
The main advantages of endoscopic collection include:
- Patient comfort, universal availability, avoidance of radiation exposure.
- Safe, easy and highly accurate, cost effective procedure ( 30% lower than traditional testing)
- Can be utilized in almost all facilities that provide endoscopic procedures.
The procedure is as follows:
- The patient is placed in the left lateral decubitus position with slight head elevation. The posterior pharynx is sprayed with topical cetacaine spray. A sedation and analgesia bolus is administered according to our previously published nomogram [Table] (1). Doses based on this nomogram have not been shown to affect pancreatic secretion (2). Further sedation doses may be given if necessary for patient comfort; however, the effect of higher doses on pancreatic secretion has not been studied. After the sedation bolus, a bite-block is placed.
- Esophagogastroduodenoscopy (EGD) is performed using a standard (10mm) or thin (6mm) upper endoscope. We have tended to use the Olympus 160XP (6mm) scope for the ePFT because it optimizes patient comfort during the prolonged endoscopy; however, standard adult scopes also work well.
- During luminal examination, an intravenous (IV) test dose of synthetic secretin (human or porcine, 0.2 micrograms) is administered. After the test dose, the pulse-ox and blood pressure are monitored for 5 minutes to ensure no rapid change. An allergic reaction to synthetic Secretin has never been reported; however, this measure optimizes safety.
- Gastric fluid is aspirated as completely as possible through the scope and discarded. We recommend retroflexion to optimally aspirate fundic gastric juice.
- After gastric fluid aspiration and discard, approximately 3-5 cc of fluid should be suctioned from the post-bulbar duodenum to rinse residual gastric fluid from the suction channel.
- At time “0” a baseline collection of 3-5 cc of duodenal fluid is collected in a trap (bottle A). Also at time “0”, the full IV dose of synthetic secretin (0.2 micrograms/kg, slow push) is administered.
- Intermittent 3-5 cc fluid aspirates are obtained every 15 minutes for an hour (Bottles B at 15 minutes, C at 30 minutes, D at 45 minutes, and E at 60 minutes).
- Some general points about fluid collection:
- Fluid samples are usually easily aspirated within seconds because of the large volume of pancreatic fluid secretion following Secretin. Occasionally, fluid secretion is less voluminous (particularly in advanced chronic pancreatitis) and may require 3-5 minutes of endoscopic manipulation to obtain an adequate sample.
- We try to keep the tip of the scope in the post-bulbar duodenum throughout the entire hour-long procedure. Between collections, the scope may be allowed to rest on the pillow or gurney in a secure position with the guardrail up to minimize movement of the scope and enhance comfort.
- Occasionally, fluid is very scarce. In this case, we put the patient in a supine, reverse-trendelenburg position to maximize pooling of fluid in the second duodenum.
- Low to intermediate suction is best to minimize trauma to the mucosa—blood in the fluid may affect the bicarbonate concentration. Another practical tip is to remove the suction cap from the scope and hold it lightly on top of the channel hub during aspiration. This allows close control of the amount of suction and minimizes mucosal trauma.
- After a collection, tightly cap each specimen and put immediately on ice.
- Fluid should be kept on ice and analyzed within 6 hours (3), or may be frozen (sub zero freezer is best) and analyzed later.
- A standard, hospital laboratory auto-analyzer (e.g. Beckman-Coulter CX3 Delta model) may be used for bicarbonate concentration analysis.
- The highest bicarbonate concentration from the 5 samples is considered the peak bicarbonate (4). A peak bicarbonate <= 80 mEq/L is considered abnormal and suggestive of exocrine insufficiency.
The two-sample ePFT
We recently reported the validity of a shortened, two-sample collection method in which samples are collected at 30 and 45 minutes after secretin administration. This method retains a high sensitivity for detecting pancreatic exocrine insufficiency and is ideal for screening patients in whom there is a low suspicion of pancreatic disease. The two-sample ePFT also serves as a useful adjunct to advanced endoscopic procedures such as endoscopic retrograde cholangiopancreatography and EUS. Patients with borderline or equivocal two-sample ePFT results should be considered for the 1-hour five-sample collection method.
ERCP
If the cause of acute pancreatitis is gallstones, patients may have to have the gallbladder removed to prevent further attacks. If the bile duct is found to be enlarged, the physician may elect to perform an ERCP (endoscopic retrograde cholangiopancreatography) to drain it. An ERCP is a way for doctors to examine the pancreas, pancreatic duct, the common bile duct, and/or sphincter of Oddi. It involves passage of a long narrow tube called an endoscope used to put X-ray contrast dye into the bile and pancreas ducts. In severe cases, surgery will be required to drain the pancreatic duct or to remove part of the pancreas.
Functional EUS
A procedure that combines the “gold standard” Secretin stimulation test to evaluate pancreas function with the highly flexible imaging by endoscopic ultrasound (EUS) procedure.
The combined procedure provides for:
- Imaging of the pancreas resting prior to stimulation.
- Dynamic imaging of the pancreas after Secretin stimulation.
- Development of before and after stimulation anatomic parameters that may be used to provide additional diagnostic insights in pancreas disease.
- Monitor pancreatic fluid flow directly and visually to evaluate ductal compliance.
- Provide easy access to samples of pancreatic fluid for electrolytes, e.g. HCO3 as well as cytokines, chemokines, and genetic end marker assays.
- You are able to get visual pictures of the pancreas and ductal structures with EUS and quantitative measurement of the pancreas with Secretin stimulation from the pancreatic fluid and bicarbonate. This combined procedure will assist you in your diagnosis for early Chronic Pancreatitis or exocrine pancreas dysfunction.
Gastrinoma
ChiRhoStim® is indicated for the stimulation of gastrin secretion to aid in the diagnosis of gastrinoma. A medical professional may suggest a biochemical study called the Secretin Stimulated blood test to check for an elevated gastrin level after an infusion of secretin.
Secretin is a hormone that causes Gastrinoma’s to release more gastrin. A technician or nurse places an intravenous (IV) needle in a vein in the arm to give an infusion of secretin. A medical professional may suspect Zollinger-Ellison syndrome if blood drawn after the infusion shows an elevated gastrin level. Once a diagnosis is made, localizing the tumor is important. Most Gastrinoma are small lesions and therefore, localizing the tumor may be difficult. Some of the tests that are performed to localize the tumor include a CT scan, octreotide scan and MRI and an endoscopic ultrasound. An experienced surgeon will detect these tumors at surgery even when they are not visible on preoperative imaging tests.
SMRCP
Imaging of the pancreas has always been a challenging procedure. ERCP’s became standard of care until the incidence of post-ERCP pancreatitis and other complications arose from increased procedure rates.
This highlighted the need for a simplified and less invasive imaging procedure (Mariani, 2009). Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) has replaced Diagnostic ERCP and has been recommended by the AGA and the ACG as the first line screening test for patients with suspected pancreatic issues.
With the development of synthetic Human Secretin (ChiRhoStim®), gastroenterologists and radiologists are able to perform dynamic imaging of the pancreas. SMRCP enables providers to gain a better visualization of the main duct and side branches of the pancreas and to examine exocrine pancreatic function.
Synthetic Human Secretin works as an adjunct to a standard MRCP. The physician is able to assess the endocrine function of the pancreas in real time with Secretin MRCP. It is a valuable tool for imaging the pancreas.
This procedure has been performed and studied extensively in the United States for the past 12 years and at least 20 years in Europe. There are over 100 medical journal articles on Secretin enhanced MRCP.
There are clearly identifiable benefits of improving visualization of the pancreas. S-MRCP has been mentioned and discussed at various medical conferences, including Digestive Disease Week, ACG Annual Meeting, the Society for Gastrointestinal Radiologist, the Radiology Society of North America, the American Pancreatic Association, and various other regional courses sponsored by the ACG and AGA.